When Do You Do Follow Up Colostomy for Family History of Colon Cancer
Following treatment for either colon or rectal cancer, ongoing follow-up to detect recurrent illness is considered an of import part of patient care for colorectal cancer. Colorectal cancer follow-up refers to a systematic approach to monitoring patients for new or recurrent cancer after treatment. The majority of these recommendations apply to both colon and rectal cancers. Differences are noted where advisable. Adherence to these guidelines can exist useful in early detection of pre-cancerous polyps and cancer recurrence. However, systematic follow-up is not foolproof and does not guarantee a new colon cancer volition not occur. The information in this brochure is intended to help patients and their families understand their connected risks for recurrent cancer and to aid guide appropriate follow-up care to maintain their cancer-free state. This document may also be of employ to treating clinicians to help guide appropriate long-term later-intendance. Each patient's intendance must ultimately exist evaluated individually. Any questions or issues related to appropriate follow-upward on an individual basis should be reviewed by the patient's treating medico, often in consultation with a colorectal surgeon or other specialist.
Patients with a history of colon or rectal cancer demand information regarding:
- Which patients need follow-up testing
- The risk of recurrent colorectal cancer
- The types and timing of appropriate follow-upwardly tests
- The signs and symptoms of cancer recurrence
- The risk of developing new polyps
- Increased family risk of polyps and colon cancer
The post-obit information outlines the general guidelines for follow-up after handling for colon or rectal cancer.
WHICH PATIENTS NEED TESTING?
Once a patient has been diagnosed and treated for colorectal cancer, it is of import to understand that connected follow-up is needed. Compared with patients with no history of colon or rectal cancer, patients with a history of colorectal cancer are at significantly increased run a risk for not but colon cancer recurrence, simply also the development of new polyps, which are the precursor lesions to colorectal cancers.
Any patient who has had curative surgery for a polyp or colorectal cancer has approximately double the take a chance for developing new polyps. These patients need to have their starting time colonoscopies 1 twelvemonth later surgery, a follow-up colonoscopy iii years afterward, and subsequent colonoscopies at no less than five-year intervals. If whatsoever new polyps or lesions are found, patient surveillance should be modified accordingly.
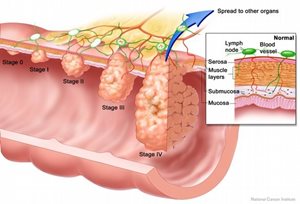
The risk of colorectal cancer recurrence can oftentimes be adamant by the stage of the cancer. Stage I cancers accept the lowest risk of cancer recurrence while stage II and III cancers have a higher risk of recurrence. Stage II cancers are those that do not have any lymph nodes involved, but the tumors grew deeper through the wall of the colon or rectum or invaded into other organs that are removed at the time of surgery. Stage III cancers refer to those that have spread to the lymph nodes. Stage 4 tumors have spread to organs distant from the colon or rectum such every bit the liver, lungs or brain (come across figure below). Due to the individual differences in Stage 4 tumors, patients follow a more individualized follow-upward routine.
HOW DO COLON AND RECTAL CANCERS RECUR?
Two master patterns of colorectal cancer recurrence are local and afar. Local recurrence refers to tumors recurring in the same area as the original tumor. Afar recurrence (metastatic illness) ways cells from the original cancer have spread to distant organs, almost often the liver or the lungs. Follow-upward tests are aimed at detecting recurrent disease in these 2 main categories.
In add-on, new colorectal cancers can develop at sites in the colon and rectum distinct from the place of the original tumor. This is not truly a recurrence, but rather a new cancer that develops one-time after the handling of the original cancer.
FOLLOW-Upward TESTING
Appropriate follow-up testing is key to the early on detection and potentially successful management of cancer recurrence. These tests have been designed in order to attempt to choice up recurrences earlier the development of symptoms, so that intervention tin can exist as successful as possible. The broad categories of follow-upwardly testing include routine medical history and concrete exam, claret tests such as serum carcinoembryonic antigen (CEA), colonoscopy, and radiologic imaging.
MEDICAL HISTORY AND PHYSICAL Examination
A medical history and physical examination are the nigh basic components of post-operative follow-upwards. While important, it is often the least effective way to observe early recurrences, because the vast majority of these practice non have any signs or symptoms. These exams are most frequently performed by the cancer patient's primary intendance physician or cancer specialist. A careful medical history may elicit new changes in bowel habits or the presence of new haemorrhage, or maybe unexplained weight loss. Any of these signs or symptoms should prompt a thorough workup. Pertinent physical test findings may include the presence of rectal bleeding or a palpable mass. Abnormal lymph node enlargement may exist felt in the groin lymph nodes, or more rarely masses may be felt during abdominal or rectal examination.
Carcinoembryonic antigen (CEA) is a protein that is made by some cancers cells, including colorectal cancer cells, and is secreted into the blood stream.
CEA blood levels should be checked around the time of surgery and approximately every 3 months subsequently treatment for at least ii years in patients who take Stage II or III colon or rectal cancer. Subsequently a 2-twelvemonth follow-up the CEA claret level is checked at least every 6 months for an additional iii years.
Elevated levels may prompt additional workup such as imaging, with a CT scan of the breast, abdomen and pelvis or a PET scan. Imaging may reveal the source of the recurrence, but occasionally may yield other incidental findings that may warrant workups.
CT SCANNING
A computed tomography (CT) scan is a very sensitive 10-ray examination that allows physicians to run into "inside" the body to place new or recurrent tumors. Almost patients who take had stage II or III colon or rectal cancer undergo yearly CT scans of the chest, abdomen, and pelvis.
COLONOSCOPY, SIGMOIDOSCOPY, AND PROCTOSIGMOIDOSCOPY
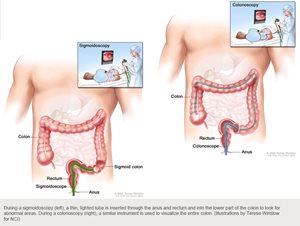
Colonoscopy and sigmoidoscopy are tests that allow the doctor to examine the entire colon or lower third of the colon, respectively. Flexible lighted cameras are inserted through the anus or through a colostomy to allow the physician to see the inside the bowel, to have pictures and biopsies, and to remove polyps. This procedure is usually performed as an outpatient at a surgery or endoscopy center. Patients are commonly required to undergo bowel-cleansing procedures for 1 or 2 days prior to the procedure, so that the lining of the colon and rectum is clean and the entire area can be seen clearly.
Proctosigmoidoscopy tin be performed with either a flexible or rigid (straight) scope. In this process, the scope is simply advanced as far every bit the lowest portion of the colon. It is used in cases when the area to exist examined is just the lower portion of the gastrointestinal tract.
Colonoscopy and flexible proctosigmoidoscopy are very safe procedures and rarely have serious complications. The 2 major risks associated with these procedures are significant bleeding and perforation of the colon. While they are of business organization, in reality, they are rare, occurring in less than 1 or 2 of every 1,000 colonoscopies.
In some patients, genetic syndromes may cause their colorectal cancer. In these unique circumstances, screening or surveillance guidelines may be much more aggressive. Decisions regarding frequency of colonoscopy should be fabricated in close consultation with your dr. and may involve follow-up with a genetics counselor.
OTHER TESTS
Rectal ultrasound is a examination sometimes used to determine the depth of cancer invasion into the rectal wall for patients with rectal cancer. It is usually administered in the office or a procedure center. Information technology may exist performed by a radiologist, colorectal surgeon, or gastroenterologist. After a cleansing enema, the test is ordinarily performed with a rigid ultrasound probe or in conjunction with a flexible sigmoidoscopy.
Positron emission tomography (PET) scanning is a radiology test sometimes used to assess the potential for tumors to spread. For this test, a special, radioactively labeled form of glucose (sugar) is injected prior to scanning, and similar to a CT scan, the patient is placed in the PET scanner. Tumors and metastases will take up the glucose faster than other tissues, and announced as bright spots on a PET scan. This test is minimally invasive and very safe. The corporeality of radiation from the injected glucose is essentially harmless, and the examination does not usually involve injection of any other dyes. Patients who are pregnant or program to have children should discuss fertility problems with their doc prior to radiation exposure.
Magnetic resonance imaging (MRI) is some other radiology test used to generate an epitome of a patient's internal anatomy. Instead of using radiation, equally a CT scan or 10-ray does, images are based on the generation of a strong magnetic field. The images obtained in this manner can provide very specific anatomic particular, which can complement the information obtained through CT scans. MRI is commonly a safe examination, just it tin be disconcerting for some patients, especially those with claustrophobia, because information technology involves beingness placed in a relatively narrow tunnel-like machine, often for 20 to 30 minutes. Patients are able to speak and interact with the technicians administering the test, just need to exist able to go along very notwithstanding. Patients with certain metallic implants such every bit pacemakers may not be able to undergo MRI.
LOCAL RECURRENCE
Local recurrence is defined equally colorectal cancer regrowing at the site of the original cancer. Since the original tumor was removed, along with the section of colon or rectum in which it arose, true local recurrence in the inner lining of the bowel may occur at the site of reconnection of the two pieces of intestine. These tumors may be visible inside the colon walls on colonoscopy equally growths at or shut to the reconnection site. They may grow into the inner lining of the bowel and crusade symptoms related to bleeding or narrowing of the connection site.
If the narrowing is significant, patients may develop changes in bowel habits (less frequent bowel movements, narrower stools, difficulty pushing out the stool) or obstructive symptoms (absent bowel movements, abdominal pain, increase in size of abdomen, airsickness). Any changes in bowel habits in a patient with a previous colon or rectal resection should be reported to their medico, and likely will need to be evaluated with a colonoscopy. With early recurrences, the tumor may not cause any symptoms at all and may only be found during routine surveillance.
Local recurrences may also occur exterior the bowel wall. These recurrences are often initially asymptomatic and non detectable past colonoscopy, since simply the within of the bowel is visible on a colonoscopy. These recurrences are unremarkably detected either by surveillance 10-rays (e.g., CT scan) or are signaled past an increase in the CEA level (meet beneath). When these outside local recurrences grow into certain structures, they may cause secondary symptoms, such every bit pain, or symptoms from other organ systems that they invade. Recurrences outside of the colon causing symptoms are often associated with a poor event.
DISTANT RECURRENCE
Afar recurrences occur in patients with delayed metastatic affliction (spread to other organs non in direct contact with initial tumor, near often through lymph nodes or the blood stream). The nigh common sites for distant recurrence of colon and rectal cancer are the liver and the lungs. These recurrences ofttimes exercise non have any symptoms and are merely found during routine follow upwards 10-rays or abnormal CEA testing which prompts imaging to look for the possible source.
WHAT HAPPENS IF RECURRENCE IS FOUND?
If a recurrence is establish during regular follow-up, your cancer specialist and your colorectal surgeon will work together to determine how extensive it is. Well-nigh likely, imaging tests, such as a CT scan or PET scan will be performed to decide whether at that place has been additional distant spread. If the recurrence is afar from the original tumor, or in more than one area, this is usually treated initially with chemotherapy. If the recurrence is local, it may be possible to treat it with some other surgery. If your original cancer was in the colon (not the rectum), it is more probable that this local recurrence will exist able to be removed.
If the local recurrence is in the rectum, this can pose specific problems when adjacent structures are involved. Attempts at surgery for cure may involve the need for removal of a portion of the sacrum (tailbone), parts of the urinary system, and vagina. In social club to decide if other organs are involved, ordinarily an MRI of the pelvis is obtained. In addition, if the patient hasn't already received radiation before their rectal cancer surgery, it is almost ever indicated in the treatment of recurrent rectal cancer.
The table below is from the American Society of Clinical Oncology website, and represents the most updated version of recommendations, based on the most contempo review of the literature on the discipline.
| Follow-Up Care Recommendations | Year i | Year ii | Twelvemonth 3 | Year iv and 5* |
|---|---|---|---|---|
| Doctor'southward Visit | Every three to vi months | Every 3 to 6 months | Every 3 to 6 months | Every 6 months |
| CEA exam | Every 3 months | Every 3 months | Every 3 months | Every bit adamant by your md |
| CT scan (chest and belly) | Every year, if recommended by your medico | Every twelvemonth, if recommended by your doctor | Every year, if recommended past your doctor | As determined by your doc |
| CT scan (pelvis) (rectal cancer simply) | Every yr, if recommended by your doctor | Every twelvemonth, if recommended by your md | Every year, if recommended by your doctor | As adamant by your doctor |
| Colonoscopy | Once | At 3 years | ||
| Proctosigmoidoscopy (rectal cancer only) | Every 6 months for five years |
*Later on 5 years, the demand for future tests and visits are decided by the patient and medico.
WHAT IS A COLON AND RECTAL SURGEON?
Colon and rectal surgeons are experts in the surgical and not-surgical treatment of diseases of the colon, rectum, and anus. They take completed advanced surgical training in the treatment of these diseases, equally well every bit general surgical training. They are well versed in the handling of both benign and cancerous diseases of the colon, rectum, and anus and are able to perform routine screening examinations and surgically care for weather, if indicated to practise so.
DISCLAIMER
The American Club of Colon and Rectal Surgeons is dedicated to ensuring high-quality patient care by advancing the science, prevention and direction of disorders and diseases of the colon, rectum and anus. These brochures are inclusive but not prescriptive. Their purpose is to provide information on diseases and processes, rather than dictate a specific class of treatment. They are intended for the utilize of all practitioners, health intendance workers and patients who desire information well-nigh the management of the weather addressed. Information technology should be recognized that these brochures should not be deemed inclusive of all proper methods of care or exclusive of methods of care reasonably directed to obtain the aforementioned results. The ultimate judgment regarding the propriety of any specific process must be made by the md in calorie-free of all the circumstances presented by the private patient.
Citations
Dujovny N and Hourigan J. Chapter 48, "Colorectal Cancer: Surveillance". Chapter in Beck DE, Roberts PL, Saclarides TJ, Senagore AJ, Stamos MJ, Wexner SD, Eds. ASCRS Textbook of Colon and Rectal Surgery, second edition. Springer, New York, NY; 2011.
ASCRS: Practice Parameters for the Surveillance and Follow-up of Patients With Colon and Rectal Cancer. Dis Colon Rectum 2004; 47: 807–817.
The website of the U.s.a. National Cancer Establish (accessed Aug 2012): http://www.cancer.gov/cancertopics/types/colon-and-rectal
© 2015 American Society of Colon & Rectal Surgeons
Source: https://fascrs.org/patients/diseases-and-conditions/a-z/colon-and-rectal-cancer-follow-up-care-expanded-ve
0 Response to "When Do You Do Follow Up Colostomy for Family History of Colon Cancer"
Enregistrer un commentaire